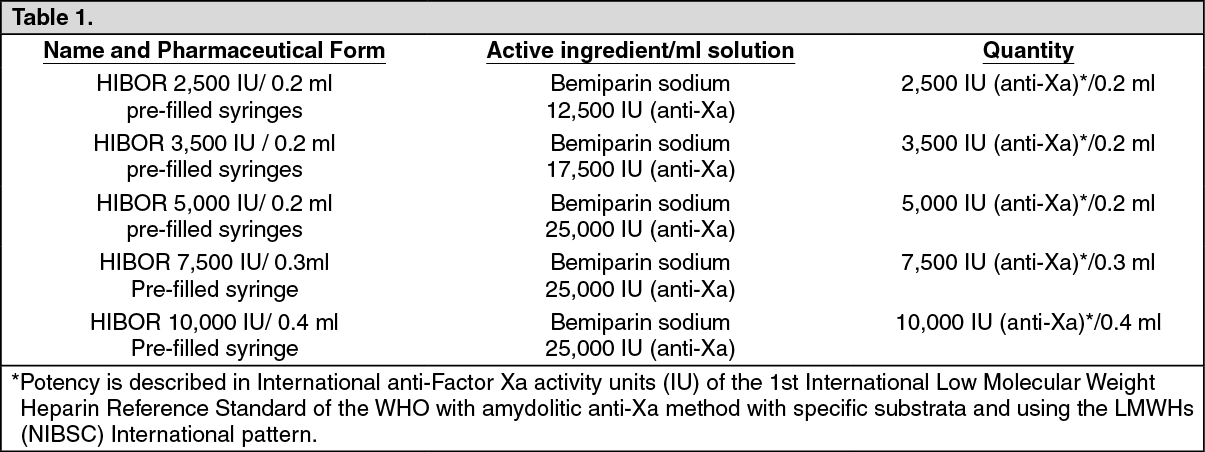
See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Bemiparin sodium is derived from porcine intestinal mucosa.
Excipients/Inactive ingredients: Water for injections.
Pharmacotherapeutic group: antithrombotic agent, heparin group. Antithrombotic. ATC code: B01AB12.
Pharmacology: Pharmacodynamics: Bemiparin sodium is a LMWH obtained by depolymerization of heparin sodium from porcine intestinal mucosa. Its mean molecular weight (MW) is approximately 3,600 daltons. The percentage of chains with MW lower than 2,000 daltons is less than 35%. The percentage of chains with MW from 2,000 to 6,000 daltons ranges between 50-75%. The percentage of chains with MW higher than 6,000 daltons is less than 15%.
The anti-Xa activity ranges between 80 and 120 anti-Xa IU per mg and the anti-IIa activity ranges between 5 and 20 anti-IIa IU per mg, calculated in relation to dry matter. The anti-Xa/anti-IIa ratio is approximately 8.
In animal experiment models, bemiparin has shown antithrombotic activity and moderate haemorrhagic effect.
In humans, bemiparin has confirmed its antithrombotic activity and, at the recommended doses, it does not significantly prolong global clotting tests.
Pharmacokinetics: The pharmacokinetic properties of bemiparin have been determined by measuring the plasma anti-Xa activity using the amydolitic method; it is based on reference to the W.H.O. First International Low Molecular Weight Heparin Reference Standard LMWH (NIBSC).
The absorption and elimination processes follow a linear kinetic of the 1st order.
Absorption: Bemiparin sodium is rapidly absorbed following subcutaneous injection and the bioavailability is estimated to be 96%. The maximum plasma anti-Xa effect at prophylactic doses of 2,500 IU and 3,500 IU occurs 2 to 3 hours after subcutaneous injection of bemiparin, reaching peak activities in the order of 0.34 ± (0.08) and 0.45 ± (0.07) IU anti-Xa/ml, respectively. Anti-IIa activity was not detected at these doses. The maximum plasma anti-Xa effect at treatment doses of 5,000 IU, 7,500 IU, 10,000 IU and 12,500 IU occurs 3 to 4 hours after subcutaneous injection of bemiparin, reaching peak activities in the order of 0.54 ± (0.06), 1.22 ± (0.27), 1.42 ± (0.19) and 2.03 ± (0.25) IU anti-Xa/ml, respectively. Anti-IIa activity of 0.01 IU/ml was detected at doses of 7,500 IU, 10,000 IU and 12,500 IU.
Elimination: Bemiparin administered in the dose range of 2,500 IU to 12,500 IU has an approximate half-life of between 5 and 6 hours, and should therefore be administered once daily.
There are currently no data available with regards to plasma protein binding, metabolism and excretion of bemiparin in humans.
Toxicology: Preclinical safety data: Preclinical data for bemiparin reveal no special hazard for humans based on conventional studies of safety pharmacology, single and repeated dose toxicity, genotoxicity and reproduction toxicity.
Acute and repeated dose toxicity studies following subcutaneous administration of bemiparin in animals have revealed alterations consisting essentially in reversible, dose-dependent haemorrhagic lesions at the injection site. These were considered to result from exaggerated pharmacological activity.
In the studies of reproductive toxicity performed with bemiparin in pregnant rats and rabbits, between days 6 and 18 of the pregnancy, no mortality was recorded among the females treated with bemiparin. The main clinical signs recorded were subcutaneous haematomas that were attributable to a pharmacological effect of the test item. No treatment-related embryotoxic effect neither external, skeletal and/or visceral alterations were recorded in the examination of fetuses.
HIBOR 2,500 IU anti Xa/0.2 ml solution for injection in pre-filled syringes.
HIBOR 3,500 IU anti Xa/0.2 ml solution for injection in pre-filled syringes.
Prevention of thromboembolic disease in patients undergoing general and orthopedic surgery.
Prevention of thromboembolic disease in non-surgical patients with high or mild risk.
Secondary prevention of venous thromboembolism recurrences in patients with deep vein thrombosis and transitory risk factors.
Prevention of clotting in the extracorporeal circulation circuit during haemodialysis.
HIBOR 5,000 IU anti Xa/0.2 ml solution for injection in pre-filled syringes.
HIBOR 7,500 IU anti Xa/0.3 ml solution for injection in pre-filled syringes.
HIBOR 10,000 IU anti Xa/0.4 ml solution for injection in pre-filled syringes.
Treatment of established deep vein thrombosis, with or without pulmonary embolism.
WARNING: The different low molecular weight heparins are not necessarily equivalent. Therefore compliance with the dosage regimen and the specific method of use for each of these medicinal products is required.
Adults: General surgery with moderate risk of venous thromboembolism: On the day of the surgical procedure, 2,500 IU anti-Xa is to be administered by subcutaneous route (sc), 2 hours before or 6 hours after surgery. On subsequent days, 2,500 IU anti-Xa sc is to be administered every 24 hours.
Orthopedic surgery with high risk of venous thromboembolism: On the day of the surgical procedure, 3,500 IU anti-Xa is to be administered by sc route, 2 hours before or 6 hours after surgery. On subsequent days, 3,500 IU anti-Xa sc is to be administered every 24 hours.
Prophylactic treatment must be followed in accordance with the physician's opinion during the period of risk or until the patient is mobilised. As a general rule, it is considered necessary to maintain prophylactic treatment for at least 7 - 10 days after the surgical procedure and until the risk of thromboembolic disease has decreased.
Prevention of thromboembolic disease in non-surgical patients: The recommended posology of bemiparin is 2,500 IU/day or 3,500 IU/day by sc route, according to whether the set of risk factors of the patient defines as mild or high thromboembolic risk.
Prophylactic treatment should be continued, in accordance with the physician’s opinion, during the period of risk or until the patient is mobilised.
Secondary prevention of the venous thromboembolism recurrences in patients with deep venous thrombosis and transitory risk factors: HIBOR may be administered at the fixed dose of 3,500 IU / day, up to a maximum period of 3 months, in patients who have received anticoagulant treatment for deep vein thrombosis with or without pulmonary embolism, as therapeutic alternative to oral anticoagulant administration or in cases of contraindication of its use.
Prevention of clotting in the extracorporeal circulation circuit during haemodialysis: For patients undergoing repeated haemodialysis sessions of no longer than 4 hours in duration and with no risk of bleeding, the prevention of clotting in the extracorporeal circulation circuit is obtained by injecting a single dose in the form of bolus into the arterial line at the beginning of the dialysis session. For patients weighing less than 60 kg, the dose to be administered will be 2,500 IU, whereas for patients weighing more than 60 kg, the dose to be administered will be 3,500 IU.
Treatment deep vein thrombosis: HIBOR should be administered by subcutaneous route at the fixed dose of 115 IU anti-Xa/kg weight/day, during 7 ± 2 days as a general rule. This daily dose generally corresponds, depending on the body weight, to the ranges: <50 kg, 0.2 ml (5,000 IU anti-Xa); 50-70 kg, 0.3 ml (7,500 IU anti-Xa); 70-100 kg, 0.4 ml (10,000 IU anti-Xa) and 100-120 kg, 0.5 ml (12,500 IU anti-Xa). In patients of > 120 kg of weight, the dose to be administered must be adjusted to the weight, at a rate of 115 IU anti-Xa/kg/day, considering the concentration of 25,000 IU / ml.
Unless contraindicated, oral anticoagulant treatment will be initiated between days 3-5 after starting the administration of HIBOR, in doses adjusted to maintain the INR between 2 and 3 on the control value. The administration of bemiparin may be discontinued once reached the mentioned value of INR. Oral anticoagulation should be continued during a minimum of 3 months.
In patients with deep vein thrombosis and transitory risk factors, as a therapeutic alternative to oral anticoagulant administration or in cases of contraindication of its use, HIBOR may be administered at the fixed dose of 3,500 IU / day, up to a maximum of 3 months.
Children: HIBOR is not recommended for use in children under 18 years due to a lack of data on safety and efficacy.
Elderly: No dose adjustment required.
Renal and hepatic impairment: There are insufficient data to recommend a dose adjustment of bemiparin in this group of patients.
Method of administratio: Subcutaneous injection technique: The patient should follow these steps: Wash hands thoroughly. The patient should be sitting or lying in a comfortable position at the time of Hibor administration.
The administration of HIBOR by subcutaneous route is performed by injecting the syringe in the subcutaneous cell tissue of the anterolateral or posterolateral abdominal waist, to 5 centimetres from the navel and any scar or bruise. Clean the skin in that area.
Use different places for the injection on different days, for example, first on the left hand side, next time on the right.
Pull the needle cap off the HIBOR syringe.
To keep the needle sterile, make sure it doesn't touch anything.
This pre-filled syringe is now ready for use.
Before injecting, do not push the plunger to get rid of any air bubbles, because the patient might lose the medicine.
Hold the syringe in one hand and with the other hand, using the forefinger and thumb, gently pinch the area of skin which the patient has cleaned and make a skin fold.
Insert the whole needle into the folded skin keeping the syringe as straight as possible on the body surface at a 90° angle.
Press down on the plunger, making sure the patient holds the skin fold in position throughout the injection.
Remove the syringe from the injection site keeping the finger on the plunger rod and syringe straight. Let go of the skin fold.
Immediately discard the syringe throwing it into the sharps bin closest (the needle in), close the container lid tightly and place it out of reach of children.
Warnings: Do not reuse the needle shield after injection.
Do not rub the skin where the patient has put the injection in. This will help to avoid bruises.
Bleeding is the main symptom of overdosage. If bleeding occurs bemiparin should be discontinued depending on the severity of the haemorrhage and the risk of thrombosis.
Minor haemorrhages rarely need specific treatment. In case of major haemorrhages, administration of protamine sulphate may be needed.
The neutralisation of bemiparin with protamine sulphate has been studied in-vitro and in-vivo systems, with the aim of observing the reduction of anti-Xa activity and the effect on the Activated Partial Thromboplastin Time (APTT). Protamine sulphate exerts a partial decrease on anti-Xa activity for 2 hours after its intravenous administration, at a dose of 1.4 mg of protamine sulphate each 100 IU anti-Xa administered.
Hypersensitivity to bemiparin sodium, heparin or substances of porcine origin.
History of confirmed or suspected immunologically mediated heparin induced thrombocytopenia (HIT) (see Precautions).
Active haemorrhage or increased risk of bleeding due to impairment of haemostasis.
Severe impairment of liver or pancreatic function.
Injuries to or operations on the central nervous system, eyes and ears within the last 2 months.
Disseminated Intravascular Coagulation (DIC) attributable to heparin-induced thrombocytopenia.
Acute bacterial endocarditis and slow endocarditis.
Organic lesions susceptible of bleed (e.g.: active peptic ulcer, haemorrhagic stroke, cerebral aneurysm or cerebral neoplasms).
Do not administer by the intramuscular route.
Due to the risk of haematoma during bemiparin administration, the intramuscular injection of other agents should be avoided.
Caution should be exercised in cases of liver or renal failure, uncontrolled arterial hypertension, history of gastro-duodenal ulcer disease, thrombocytopenia, nephrolithiasis and/or urethrolithiasis, choroid and retinal vascular disease, or any other organic lesion susceptible of bleed, or in patients undergoing spinal or epidural anaesthesia and/or lumbar puncture.
Bemiparin, like other LMWHs, can suppress adrenal secretion of aldosterone leading to hyperkalaemia, particularly in patients such as those with diabetes mellitus, chronic renal failure, pre-existing metabolic acidosis, a raised plasma potassium or those taking potassium sparing drugs. The risk of hyperkalemia appears to increase with the duration of therapy but is usually reversible (see Adverse Reactions). Serum electrolytes should be measured in patients at risk before starting bemiparin therapy and monitored regularly thereafter particularly if treatment is prolonged beyond 7 days.
Occasionally a mild transient thrombocytopenia (type I) at the beginning of therapy with heparin with platelet counts between 100,000/mm3 and 150,000/mm3 due to temporary platelet activation has been observed (see Adverse Reactions). As a general rule, no complications occur and therefore treatment can be continued.
In rare cases antibody-mediated severe thrombocytopenia (type II) with platelet counts clearly below 100,000/mm3 has been observed (see Adverse Reactions). This effect usually occur within 5th to 21st day after the beginning of treatment, although in patients with a history of heparin-induced thrombocytopenia this may occur sooner.
Platelet counts are recommended before administration of bemiparin, on the first day of therapy and then regularly 3 to 4 days and at the end of therapy with bemiparin. In practice, treatment must be discontinued immediately and an alternative therapy initiated if a significantly reduced platelet count is observed (30 to 50 %), associated with positive or unknown results of in-vitro tests for anti-platelet antibody in the presence of bemiparin, other LMWHs and /or heparins.
As with other heparins, some cases of cutaneous necrosis, sometimes preceded by purpura or painful erythematous blotches have been reported with bemiparin (see Adverse Reactions). In such cases, treatment should be discontinued immediately.
In patients undergoing epidural or spinal anesthesia or lumbar puncture, the administration of heparin with prophylactic use may very rarely be associated with epidural or spinal haematoma, resulting in prolonged or permanent paralysis (see Adverse Reactions). The risk is increased by the use of an epidural or spinal catheter for anesthesia, by the concomitant administration of drugs with action in the coagulation such as nonsteroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors or anticoagulants (see Interactions), and by traumatic or repeated puncture.
When reaching a decision as to the interval between the last heparin administration at prophylactic doses and the placement or removal of an epidural or spinal catheter, the product characteristics and the patient profile should be taken into account. The subsequent dose of bemiparin should not take place until at least four hours after removal of the catheter. The subsequent dose should be delayed until the surgical procedure is completed.
Should a physician decide to administer anticoagulation treatment in the context of epidural or spinal anaesthesia, extreme vigilance and frequent monitoring must be exercised to detect early any signs and symptoms of neurological impairment, such as back pain, sensory and motor deficits (numbness and weakness in lower limbs) and bowel or bladder dysfunction. Nurses should be trained to detect such signs and symptoms. Patients should be instructed to inform a nurse or a clinician immediately if they experience any of the previously mentioned symptoms.
If signs or symptoms of epidural or spinal haematoma are suspected, urgent diagnosis and treatment including spinal cord decompression should be initiated.
Effects on ability to drive and use machines: HIBOR has no influence on the ability to drive and use machines.
Pregnancy: Animal studies have not shown any evidence of teratogenic effects with the use of bemiparin (see Pharmacology: Toxicology: Preclinical safety data under Actions). For bemiparin, no clinical data on exposed pregnancies are available. Therefore, caution should be exercised when prescribing to pregnant women.
It is unknown whether bemiparin crosses placental barrier.
Lactation: Insufficient information is available as to whether bemiparin passes into breast milk. Therefore, where it is necessary for lactating mothers to receive HIBOR, they should be advised to avoid breast-feeding.
The most commonly reported adverse reaction is haematoma and/or ecchymosis at the injection site, occurring in approximately 15% of patients receiving HIBOR.
Osteoporosis has been associated with long-term heparin treatment.
The undesirable effects are listed by system organ class and frequency: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data).
The frequency of adverse events (AEs) reported with bemiparin is similar to those reported with other LMWHs and is as follows: See Table 2.
Click on icon to see table/diagram/image
Bemiparin sodium interactions with other medicinal products have not been investigated and the information given on this section is derived from data available from other Low Molecular Weight Heparin.
The concomitant administration of bemiparin and the following medicinal products is not advisable: Vitamin K antagonists and other anticoagulants, acetyl salicylic acid and other salicylates and NSAIDs, ticlopidine, clopidogrel and other platelet inhibitors systemic glucocorticoids and dextran.
All these drugs increase the pharmacological effect of bemiparin by interfering with its action on coagulation and/or platelet function and increasing the risk of bleeding.
If the combination cannot be avoided, it should be used with careful clinical and laboratory monitoring.
Medicinal products that increase the serum potassium concentration should only be taken concomitantly under especially careful medical supervision.
Interaction of heparin with intravenous nitroglycerine (which can result in a decrease in efficacy) cannot be ruled out for bemiparin.
Incompatibilities: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Special precautions for disposal: Single-dose container. Discard any unused content. Do not use if the protective package is opened or damaged. Only clear colourless or slightly yellowish solutions, free of visible particles, should be used.
Any unused product or waste material should be disposed of in accordance with local requirements.
Do not store above 30°C. Do not freeze.
Shelf-life: 2 years.
After first opening, HIBOR should be used immediately.
B01AB12 - bemiparin ; Belongs to the class of heparin group. Used in the treatment of thrombosis.
Hibor 2500/3500/5000/7500/10000 IU soln for inj 10,000 anti-Xa IU/0.4 mL
10 × 1's;2 × 1's
Hibor 2500/3500/5000/7500/10000 IU soln for inj 2,500 anti-Xa IU/0.2 mL
10 × 1's;2 × 1's
Hibor 2500/3500/5000/7500/10000 IU soln for inj 3,500 anti-Xa IU/0.2 mL
10 × 1's;2 × 1's
Hibor 2500/3500/5000/7500/10000 IU soln for inj 5,000 anti-Xa IU/0.2 mL
10 × 1's;2 × 1's
Hibor 2500/3500/5000/7500/10000 IU soln for inj 7,500 anti-Xa IU/0.3 mL
10 × 1's;2 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image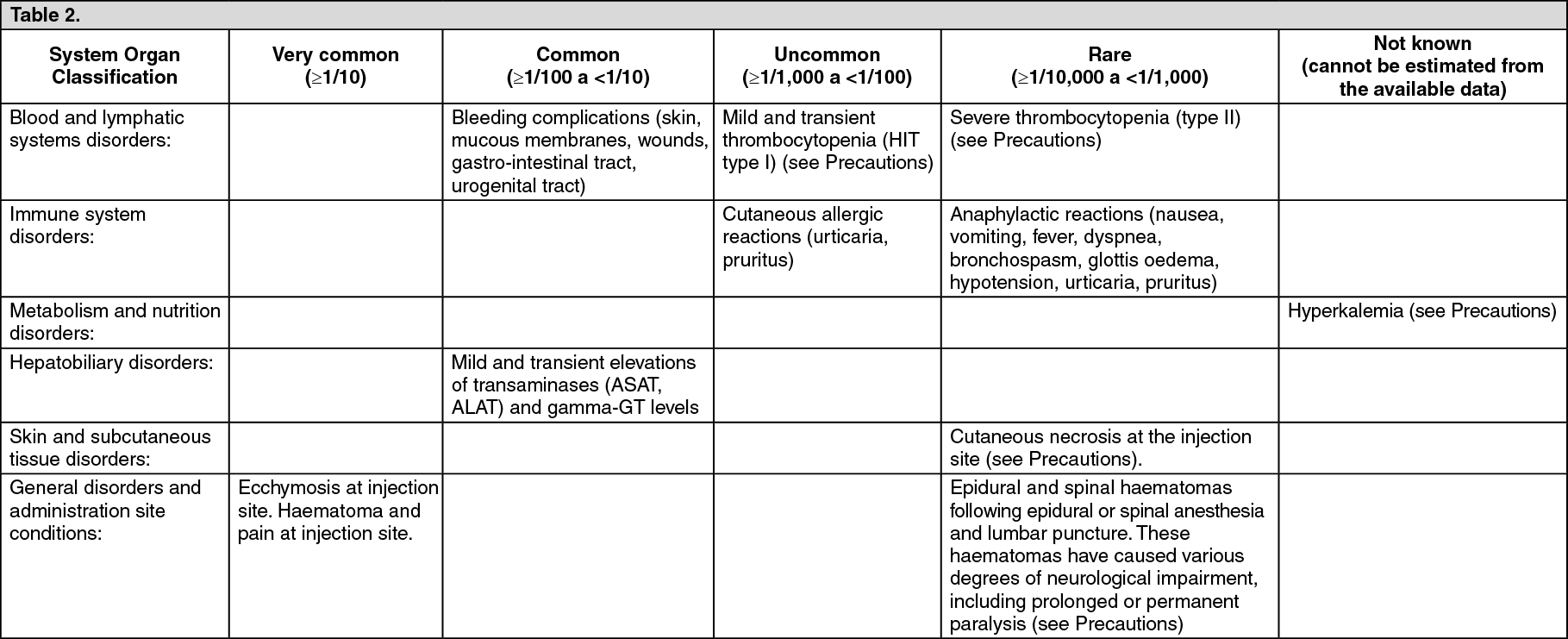 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image





 Sign Out
Sign Out